Cannabis / Marijuana / Hashish /গাঁজা / ভাঙ্

General features: Cannabis is perhaps the most debatable herb ordinarily known as marijuana or hashish all around the globe. It enables to exert impermanent psychotic or euphoric effect that entices a great many people particularly the youths to use it for recreational purposes. In Bengal, it is titled as Ganja (গাঁজা) or Bhang (ভাঙ্). Approximately, ~ 4 % of the entire global population falling in the ranges of 15 – 64 years of age have used it in few occasions in their life time for the sake of enjoyment. Interestingly, that percentage remains unchanged even today. The world’s net legal production is ~ 70,000 kg / year. Cannabis or cannabinoid is counted as narcotics and a contraband product in many countries. The presence of tetra-hydro cannabinol (THC) and its various analogs are identified to be the psychoactive agents produced inside the plant. Pharmacological studies exploring its numerous physiologic functions provide wealth of information that leads to synthesize significant number of compounds which are prescribed as necessary medicines used for anti-inflammatory, analgesic, anti-psychotic and numerous other indelible diseases. The plant belongs to Cannabaceae family which fits in the genus of flowering plants. Majorly, three species of this genus naturally occur, which are Cannabis Sativa, Cannabis Indica and Cannabis Ruderalis. Cannabis Indica and Cannabis Ruderalis are occasionally considered to be the subspecies of Cannabis Sativa. All of them are the native of Indian subcontinent and Central Asia. The plant grows in sunny and temperate climatic condition thus often seen in many tropical and subtropical regions of the world. The flowering tops of plants secrete a resinous psychoactive compound commonly called cannabinoids that possesses the actual psychoactive ingredients. In recent days, some of its derivatives are used for numerous medicinal purposes. Cannabis is a fast growing annual plant. It earns maturity within 2 – 4 months under sunny and temperate condition. Cannabis Sativa grows ~ 15ft high whereas Cannabis Indica reaches only ~ 6ft in height and the other one is about the same. The plant is dioecious by nature meaning to exist in both sexes of male and female. They produce different types of flowers. The male flowers produce pollen which synthesize least amount of THC whereas the female ones are loaded with the psychoactive compounds. Several monoecious type is also known. In this category, the individual plant bears both male and female flowers botanically termed as hermaphrodite. In normal cases, female plant blooms large resin-secreting flowers. Although male plants pollinate the females initiating the seed production but the flowers which are normally consumed are the seedless females (Sinsemilla), enriched with cannabinoids including THC. The hermaphrodites or self-pollinated type produces less seedless Sinsemilla thus have a low level of cannabinoids.

As per the plant anatomy, region called Bract holds the female reproductive part looking like green tear shaped leaves which are excessively surrounded by the resin glands producing highest level of cannabinoids. Calyx is a translucent layer over the ovules situated at the base of flower. The Trichomes appear to be clear bulbous globe that offers protection to the plant against any predators. They secrete aromatic oil containing terpenes, and cannabinoids including THC and CBD. The leaves of Cannabis Sativa, Cannabis Indica and Cannabis Ruderalis are somewhat different by the appearance. For example, in Cannabis Sativa the leaves are long and slender (> 7 inches long) having pockmarks and rough edges displaying lime green. Its large leaf contains at least 13 leaflets.
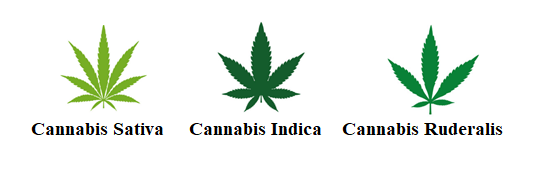
But for Cannabis Indica, the leaves are slight wider, stocky also shorter in size and have few leaflets about 7 – 9. They are deep olive green in color. The fading green coloration if appears that would signify the sign of malnourishment. For Cannabis Ruderalis, the leaves are shorter and having 5 – 7 leaflets. Its overall look is close to Cannabis Indica but the color of leaves are less green.
Hindu mythology behind cannabis use: The medicinal use of cannabis has been extensively mentioned in Atharvaveda around ~ 2000 BC which is considered as being the earliest information revealed in history. According to the Vedas, cannabis is a source of joy and happiness which is offered to the human to lose fear and attaining delight also to remove away the anxiety. Its use in the Hindu mythology is wide spread which gives impetus to many for its use but that practice ends up as abuse. Interestingly, the use is associated with the worshipping of Lord Shiva, the hermit or nomadic hippie God scantily dressed riding on a bull who is also the sole protector and destroyer of universe, often indulged Himself in its use either by smoking Ganja (dried leaves) or eating or drinking with sweets (Bhang). The myth says that, Lord Shiva after a domestic quarrel with his wife, Parvathi left home and went inside a forest for cooling down and rest. While resting, he fell asleep under the shade of a large banyan tree. Right after waking up, He noticed beautiful plants before Him. Being curious, He chewed few leaves that provided Him extreme joy, divine pleasure and mental relaxation removing away any anxiety and anger. From then on, He included those leaves as a favorite entity for daily use. To the Hindus, cannabis is considered as a sacred plant.
Different ways of using cannabis
| Forms | Source | Ways of use / abuse |
| Marijuana / Charas / Ganja | Dry leaves, flowers and stems | Smoking as joint |
| Bhang | Fresh leaves and stems | Making foods for oral use.
|
| Hashish / oil | Leaves, stems and flowers | Smoked as joint. |
|
|
Cannabis use in other religions: Buddhism does not encourage the use of cannabis. It is considered to be an intoxicating agent that hinders meditation also clouding the mental awareness. Whereas Sufis during 13th century used cannabis for many spiritual contexts. In recent days, besides the Hindus the use of cannabis is seen only among the Sufis (particular sect preaching the mystical / spiritual representation of Islam religion) around the world especially in Pakistan, India, Turkey and Indonesia during the annual festival named Urs which usually falls on Thursday evening. Further, in old Nordic culture, Freya the love goddess of Norse often used it for enchantment as well as to enhance her pleasantness and sexual behavior. In recent days, the Rastafari movement (Jamaican variety of Christianity originated from Ethiopia) has included cannabis as a divine rite. In addition to the Rastafarian some Christian sects also use cannabis as a sacrament.
History of cannabis use: Around ~ 2000 BC or earlier, the euphoric / ecstatic property of cannabis was identified at first in India. It was recommended at the then time by the ancient apothecaries for medicinal reasons to reduce fever, inducing sleep, relieving headaches, curing venereal diseases and stimulating the appetite. About the same time (2000 – 2700 BC), the medicinal practice of cannabis was also noticed among the Chinese. They used the herb in treating rheumatic pain, malaria, constipation or female menstrual disorders. Besides the medicinal role, cannabis plants or hemp (colloquial name for non-medicinal cannabis) are employed to make ropes by the ancient Chinese, Greeks and Romans which they used for their naval purposes. The hemp rope is extremely sturdy and not easily ruptured by any natural course. Hemp is categorized as inferior grade cannabis plants which are used for the industrial and commercial reasons like, rope making, fiber or textile for weaving to produce garments. Some of the hemp products are also utilized for the preparation of food and drinks. Hemp oil from cannabis seeds are used in making oil soluble paints, creams or moisturizing agents or even spent for the cooking of foods. Hemp seeds are quite identical to flax seeds which is used as bird or animal feed. The medicinal use of cannabis was introduced in the western nations in the middle of nineteenth century (~ 1840 AD) by a British army physician, Major W. B. Shaughnessy while serving the British Indian army in India. He went through large pile of millennia old Indian medical literature and arrived at the conclusion that cannabis is a safe drug for use. Before prescribing to the human he conducted extensive experiments on various animals like rats, mice or rabbits to observe any adverse effects particularly concerning the mortality. The herb did not kill anyone even at significantly high doses. So, he started prescribing to the patients experiencing seizures, rabies, rheumatism, fevers and tetanus. In that act, he recorded the anti-convulsive, analgesic, anti-anxiety and anti-emetic role of cannabis. Through his efforts, cannabis became an acceptable medicine in England and other European nations. With the arrival of twentieth century, the medicinal use of cannabis becomes slowly disappeared due to the advent of various synthetic drugs. Further, the fear of cannabis associated with possible addiction made it forbidden to cultivate in the United States and some European nations. Although its illegal use as a recreational drug remains very rampant everywhere. Strangely, in recent days about thirty states within US along with the neighboring Canada have legalized its use and cultivation.
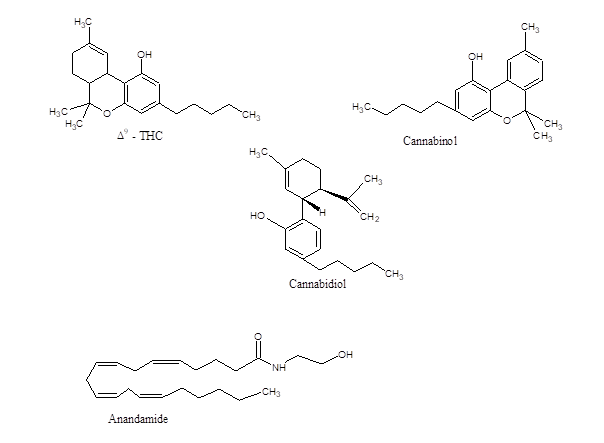
Chemical components of cannabis: Cannabis plants produce large group of terpeno-phenolic compounds which enable to induce euphoria normally experienced after consuming marijuana. Approximately 480 compounds are identified in this herb of which nearly 85 different cannabinoid components have been so far isolated and characterized. Actually, cannabinoids are named only for those C-21 compounds which are synthesized within the plant including the transformed products and related analogs. Among them, only three compounds are seen to exist at the highest level, which are cannabinol (CBN), cannabidiol (CBD) and Δ9 – tetra-hydro-cannabinol (Δ9 – THC). Interestingly, Δ9 – THC is identified to be the only psychoactive component. In majority instances CBD and Δ9 – THC are the majorly available products. The existence of CB is very low and like CBD, it has no psychoactive role.
Major ingredients of cannabis
| Psychoactive compounds | Biological effects |
| Δ9 – tetra-hydro-cannabinol
(Δ9 – THC) |
Major psychoactive component exerting psychological and
Behavioral effects. |
| Δ8– tetra-hydro-cannabinol | Less potent in psycho-activity than Δ9 – THC. |
| Cannabinol (CBN) | Much less psychoactive than Δ9 – THC. |
| 11 – hydroxyl – Δ9 – THC
(11 – OH – Δ8 – THC) |
Reason for psychological effects of cannabis. |
| Anandamide (endo-cannabinoids)
(Arachidonyl-ethanol – Amide) |
Identical to Δ9 – THC action and other cannabinoids that interact
with cannabinoid receptors. |
| Non-psychoactive compounds | Biological effects |
| Cannabidiol (CBD) | No psychoactive role but exerts anticonvulsant effect. |
| Cannabichromene
((-) Δ8 – THC -11- oic acid). |
Only analgesic action but no psychoactive role. |
|
|
Interestingly, the physiologic action of Δ9 – THC is highly stereo-selective. The (-) – trans isomer is seen much (≥ 100 times) potent than (+) – trans isomer. The presence of Δ8 – THC, a positional isomer is also seen to be effective but with less potency. Each plant produces two types of cannabinoids. For that reason, they are characterized according to their chemical phenotype / chemotype depending on the ratio of Δ9 – THC / CBD synthesized within them, which is seen to remain constant throughout the plant life. It is definitely genetically determined although environmental factor has a large impact. There are some non-drug plants which have very low level of THC but high level of CBD. Obviously the major drug-plants does the opposite by synthesizing high level of Δ9 – THC and low amount of CBD. Often the two phenotypes cross-pollinate. In that case the first Filial (F1) generation creates an intermediate while synthesizing median level of both. The female variety of this phenotype generates enough Δ9 – THC for which it could be regarded as drug producing plant therefore utilized for the drug productions. Some of the plants are seen to produce as high as 20 % Δ9 – THC. In recent days, many genetically modified plants have been developed for much larger synthesis of Δ9 – THC.
Structure activity relation and pharmacologic behavior concerning Δ9 – THC: The strong analgesic behavior of Δ9 – THC as a natural product and large content of non-steroidal compounds create colossal interest in the field of pharmacology. Extensive studies regarding the structure-activity relationship using numerous cannabinoid analogs have confirmed strict stereo-chemical requirement to exert any pharmacological effects. In fact, this information points out actual possibility for the existence of specific cannabis receptors. In the case of Δ9 – THC, it is initially speculated that there are three points of attachment needed to interact with the receptor for exerting any pharmacological actions. Those are comprised of A) phenolic group, B) proper substituent at C9 and C) a lipophilic side chain. With the idea of three point attachment and necessary involvement of dibenzo-pyran ring and lipophilic tail a few derivatives were synthesized showing strong analgesic property. One of them is CP – 55,940 (Pfizer) showing identical property like Δ9 – THC, even having ~ 50 times potent analgesic effect. Initially it was not counted to be in the category of cannabinoids. But the studies afterwards have proven that it acts as an agonist toward the cannabinoid receptors (CB1, CB2 & CB3) which can be blocked specifically by the CB1 receptor blocker acting as inverse agonist, Rimonabant (anti-obesity drug). Both CB1 and CB2 are the classic G-protein coupled receptor (GPCR) having seven transmembrane strands spanning the cell surface membrane bilayer. CP – 55,940 is a complete agonist showing high affinities, Ki ~ 0.58 nM toward CB1 and ~ 0.68 nM for the CB2. The compound also acts as an agonist toward the CB3 (called GPR55 / orphan receptor family, activated by Δ9 – THC, mostly found in liver). The compound, CP-55,940 provides neuro-protective effect by blocking the intracellular release of Ca+2 causing subsequent death of hippocampal cells during excessive exposure of N-methyl – d – aspartate (NMDA). On the other hand it induces death in cultured mouse neuroblastoma cell line, NG108-15. Further, it protects brain mitochondria from the poisoning effect of paraquat (N, N`- dimethyl – 4 – 4`- bipyridinium dichloride). Another bicyclic compound structurally differed from Δ9 – THC is Pravadoline, a non-steroidal anti-inflammatory agent with high analgesic property. Pravadoline does not work via any opiate receptors but produces powerful anti-nociception action. The compound inhibits the enzyme, cyclooxygenase (COX) thus blocking the pathway for generating pro-inflammatory molecules while producing strong analgesic effects. It is also an agonist toward the CB1 and CB2 receptors imposing anti-nociceptive actions. Concerning anti-nociception action, another cannabinoid has been synthesized, Win 55,212 -2 (Pfizer) which also behaves like Δ9 – THC.
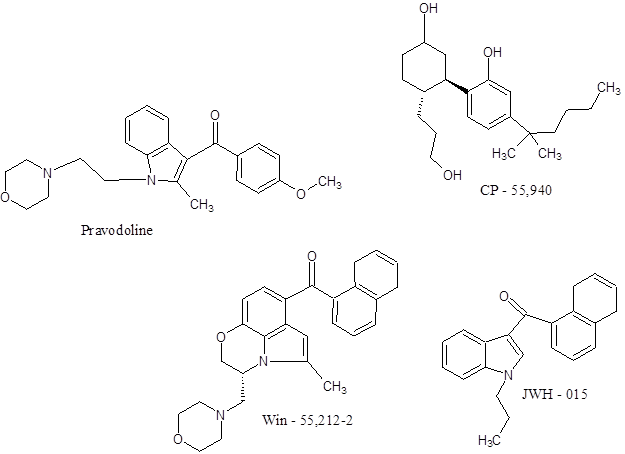
Win 55,212-2 is characterized as amino-alkyl-indole derivative. Despite having somewhat different structure, its action is identical to Δ9 – THC. It is a potent cannabinoid agonist acting as powerful analgesic thereby reducing the neuropathic pain. It also prevents cognitive impairment and the loss of neuronal markers. Like the naturally produced Δ9 – THC, it induces strong anti-inflammatory response via the receptors preventing microglial activation which elicits the neuronal inflammation. Δ9 – THC can fully eliminate the neurotoxicity caused during microglial activation. On the other hand in some cases Win 55,212-2 is seen to impair memory function and network connectivity in the brain. The compound has higher affinity toward CB1 (Ki ~ 1.9 nM) compared to Δ9 – THC (Ki ~ 41 nM) while acting as agonist. Another synthetic cannabinoid agonist is JWH – 015 (Pfizer). The compound also shows high affinity toward CB2 (Ki ~ 14 nM) than the CB1 (Ki ~ 380 nM). Besides having anti-inflammatory or analgesic effects, JWH – 015 displays strong immunomodulatory role.
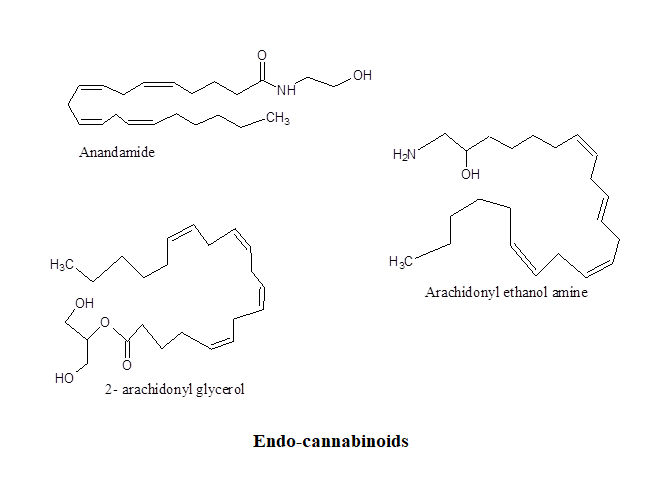
Cannabinoid receptors and physiological interaction with cannabinoids and endogenous cannabinoids (ECBs): Until now three types of cannabinoid receptors, CB1, CB2 and CB3 are identified, of which the first two are the major ones located mainly on nervous system. Their discovery provides enormous information about the physiological role of cannabinoids. Further, the finding of endogenous ligand like anandamide, Arachidonyl-ethanolamine and 2- Arachidonyl-glycerol categorized as endo-cannabinoids (ECBs) came into limelight which enhances further interests about the role of cannabis on health and diseases. The ECBs are lipid based neurotransmitters which bind to the cannabinoid receptors that are expressed normally all over the central nervous system plus brain including the peripheral nerve tissues. The ECBs are generated as per necessity especially when triggered by the increase of intracellular Ca+2 at the post-synaptic sites in response to sustaining synaptic actions. Advantageously, ECBs are rapidly metabolized after the reuptake. They are the derivatives of arachidonic acid like Arachidonyl-ethanol amine (AEA), 2- Arachidonyl glycerol (2-AG) and anandamide and act as endogenous agonists to the receptors particularly to the CB1 and CB2 displaying high affinities (Ki ~ 80 nM to 300 nM). The ECBs regulate varieties of physiological and cognitive senses, also enables to cross the blood brain barrier. Additionally, it has the role on fertility, pregnancy, appetite, mood, pain sensation, memory and pre and post-natal development. ECBs also mediate euphoria, locomotor activity, attention, and reward processes. For example, the level of anandamide soars up during physical exercise modulating motivational salience or exercised induced euphoria.
As per the CB1 receptor, it is by far the most abundant G-protein coupled receptor (GPCR) within CNS, expressing at much high level within neo-cortex, hippocampus, basal ganglia, cerebellum and brainstem. It also exists on peripheral nervous system and further on non-neuronal sites like testis, eye, spleen and vascular endothelium. The receptors are heavily expressed at the presynaptic and axonal compartments. It is directed to bind naturally synthesized ligand Δ9 – THC which mediates the physiologic effects. The receptor, CB1 also binds with several synthetic mimetics like CP55940, WIN 55,212-2, JWH -015 and ECBs acting as complete agonists. The CB1 receptor is linked to the Pertussis toxin sensitive inhibitory Gi /o protein. Thus agonist activation leads to the lowering of intracellular generation of cAMP via the inhibition of adenylate cyclase. CB1 is quite abundant in CNS having the major duty to maintain synaptic plasticity and neural transmitter release. When activated by the agonists, it sends three very different spatio-temporal waves. The initial one is transient (~ 10 mins) is caused by the activation of G proteins whereas the second wave (> 5 mins) is mediated via β – arrestins. The third and last wave takes place at intracellular compartments which may arise either by the G proteins or arrestins. Further, CB1 shows constitutive activity, an indication of G protein activation without the presence of any agonists. This effect can be reversed by the binding of inverse agonist AR141716A, commercially named Rimonabant often used as anti-obesity medication.
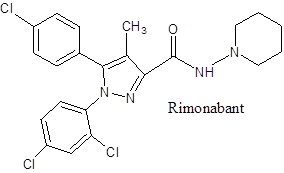
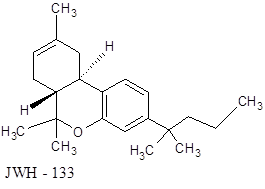
In comparison to CB1, CB2 shows more defined localization inside the brain expressing largely within the cells and tissues associated with the immune system. It exists in microglia (resident macrophages of CNS) and its expression is allied with the inflammation. Its localization on microglia is significant since it has important role in Alzheimer’s and other neural diseases connected to the basal ganglia since that controls synaptic functions and involved in the drug abuse. Further, the selective CB2 agonist JWH133 (Ki ~ 3.4 nM) inhibits dopaminergic firing from the ventral tegmental area reducing cocaine addiction. CB2 works independently to modulate inhibitory plasticity of the hippocampus. The receptor belongs to the GPCR family and attached with Gi /o. Regarding the molecular picture of ligand interaction, it is identified that lipophilic group of agonists interact with F5.46 residue of receptor that allows to form H bond with S3.31 residue imposing conformational alteration triggering the intracellular signaling pathways. Regarding the signaling process exerted by the cannabinoids several data also suggest that the receptors also can activate the Gq leading to the activation of enzyme, phospholipase C that in turn enables to cleave phosphatidyl inositol bi-phosphate (PIP2) producing inositol triphosphate (IP3) and diacylglycerol (DAG). IP3 triggers Ca+2 release from the internal stores of endoplasmic / sarcoplasmic reticulum whereas alongside DAG activates the protein kinase C. Although few disagree about this pathway suggesting no direct involvement of the cannabinoid receptor. The discovery of high affinity CB1 antagonist, SR14176A / Rimonabant positively provides evidence of cannabinoids, particularly Δ9 – THC which influences the role of other traditional neurotransmitters like dopamine (DA), acetylcholine (Ach), 5-hydroxy tryptamine (5-HT or serotonin), γ – aminobutyric acid (GABA), histamine, norepinephrine (NE), opiate peptides, prostaglandins (PGEs) and its impact on neuropharmacology. Cannabinoids enhance the synthesis of NE, DA and 5 – HT. Cannabinoids also stimulate the release of DA from corpus striatum, nucleus accumbens and prefrontal cortex. The increase of GABA level is also noticed. The major effects of cannabinoids are hypothermia, anti-nociception and change of motor activity. Catalepsy or decline of locomotor action often noticed due to cannabinoids is caused by the release of Ach and its subsequent action on muscarinic and nicotinic receptors and simultaneous release of GABA and its action on GABAA and GABAB receptors and PGEs on prostaglandin receptors. Normally, the extrapyramidal system of brain is involved in catalepsy which is further proven by injecting 11- OH- ∆8 – THC inside the pyramidal tract. The interaction of ∆9 – THC with the neuronal cells within basal ganglia also induces catalepsy. Whereas the incidence of hypothermia by the cannabinoids is mediated by the DA, NE, 5-HT, GABA, Histamine and opiate peptides which is evidenced by the experiments on animals. But the studies on hypothermia are not so consistent therefore unable to pinpoint the exact cause. The event of anti-nociception produced by cannabinoids is highly complex. It is noticed that endogenous neurotransmitters, NE, 5 – HT, ACh, GABA, opiate peptides, PGE1 and PGD2 inhibit the nociception. It is thus a possibility that some of them might interact with cannabinoids to produce the effect of anti-nociception particularly, catecholamines, PGE1, 5 – HT and opiate peptides.
Tolerance and dependence: The pharmacological role of cannabinoids establishing tolerant effect is visualized for both human and primates, rodents, dogs and few others. The tolerance is also noticed in cultured human fibroblast cells when stimulated by the cannabinoids to synthesize PGE2 and arachidonate release including the inhibition of adenylate cyclase activity. But the exact reason behind the development of tolerance remains very much unknown even today. The drug tolerance presumably happens by following the two methods. One is due to changes in pharmacokinetics whereas the other occurs owing to the changes in pharmacodynamics. Evidences indicate that the former which comprises of absorption, metabolism, distribution and excretion plays a minor role. But, the pharmacodynamic events that involves receptor downregulation, conformational alteration of receptor by binding to the agonists and subsequent internalization of ligand receptor complex is possibly the significant cause behind the development of tolerance. Studies indicate that cannabinoid tolerance is partly due to the agonist induced receptor down-regulation. Behavioral tolerance has been observed in case of chronically treated animals which shows decrease in binding in several parts of the brain like limbic forebrain (involved in controlling body temperature, eating, sleeping, emotions and reproductive functions) and striatum (involved in multiple planning and coordination) but contrarily it is enhanced in cerebellum and hippocampus. Convincing evidences exist regarding the development of tolerance toward Δ9 – THC in human like that has been noticed in the case of animals. Tolerances are noticed concerning cardiovascular effects, autonomic functions, mood changes, sleep disturbances and intra-ocular pressure when Δ9 – THC is orally administered. Whereas the results remain inconclusive regarding any behavioral changes. No behavioral alteration is observed if orally administered for low doses infrequently. A noticeable changes is seen when Δ9 – THC is taken at high doses (10 mg) orally for a long period of time. The chronic use of cannabis does not result any severe or significant withdrawal syndrome. But occasional auditory and visual hallucinations along with irritability feelings are reported. Controlled study using high doses (10 mg / dose) of Δ9 – THC administration six times a day for three weeks and its subsequent total withdrawal afterward shows restlessness, anorexia, mild nausea, irritability and sleeplessness in the behavior. Later re-administration in small doses alleviates those symptoms establishing the facts of withdrawal symptoms. Certainly there are many other factors liable for developing tolerance as well as the withdrawal effects.
Effects on central nervous system: It is certain that the major target of cannabis is brain. Therefore, most researches are directed to study its effect on the CNS. Its action on electro-encephalograph (EEG), cerebral blood flow (CBF) and brain morphology are studied over a long period of time in human, primates and animals after exposing them at various stages. According to the study, after six months of smoking marijuana, subcortical alteration of EEG among the primates has been noticed within amygdala, hippocampus and septal region, which are affected profoundly. The studies in human after acute exposure of ∆9 – THC indicates enhancement of the alpha power followed by the decrease of alpha frequency and additional decrease in beta activity which is consistent with the findings of experiencing drowsiness. Exposure of 15 – 30 years of chronic marijuana shows large increase of absolute alpha power also higher theta activity in the frontal cortex. Further, acute cannabis exposure to inexperienced users decreases global CBF however for experienced users the effect is just opposite, increase in both hemispheres but primarily in the left temporal and frontal regions. It is speculated that increased anxiety level in the case of inexperienced users may be the cause behind this decreasing effect on CBF. Increased cerebellar blood flow is correlated with the level of intoxication. Further, ∆9 – THC enhances the cerebellar metabolic rate in humans and primates. Its role in human brain is localized within specific areas eg, cerebellum and pre-frontal cortex.
Cardiovascular effect: Cannabinoids exert strong cardiovascular effects. The most effective one is ∆9 – THC which can induce tachycardia, orthostatic hypotension and prevent platelet aggregation. Noticeable changes in electrocardiogram are observed with variable P and T waves but on the other hand ST segment is somewhat decreased. The exposure to cannabinoids can aggravate angina, congestive heart failure and other preexisting conditions. Sudden high doses enhance the heart rate and reddening of body color. That appearance is due to the vasodilation of peripheral blood vessels. But after prolong exposure bradycardia and subsequent hypotension occurs. The involvement of CB1 receptor has been identified for hypotensive actions. Identical behavior has been noticed for anandamide also. But anandamide also exerts brief pressor response which is not mediated via the CB1 receptor. But the hypotensive action occurs via the inhibition of sympathetic tone mediated by the CB1.
Effect on Multiple sclerosis (MS): It is established that MS is immune-related neurodegenerative disease. It occurs due to the demyelination of neurons that inflicts dreadful pain associated with motor dysfunction as well as loss of coordination along with the severely deficient neuronal functions. The positive effects of cannabis particularly Δ9 – THC, cannabidiol (CBD) or even plant extract causes symptomatic improvement within the MS patients. It reduces the pain and associated motor dysfunction. In frequent occasions the drug, Sativex (botanical drug, mixture of CBD and THC) is recommended to treat spasticity among the MS sufferers. As per molecular mechanism, the actions take place by agonist activation of CB1 and CB2 receptors exerting anti-inflammatory and neuroprotective effects within the neurons upregulating interleukins in astroglia while reducing cytotoxic factors like nitric oxide, reactive oxygen species and pro-inflammatory cytokines in microglia. Besides the natural agonists, the use of synthetic cannabinoids (WIN 55,212-2 and JWH-015) also exert similar effects reducing pain and motor dysfunction. Presumably, in MS the neuroprotective role of CB1 and CB2 receptors are impaired so its enhancement could be the potential treatment approach.
Effect on Alzheimer’s disease (AD): The mechanism behind the action of cannabinoids on AD is not precisely known. Preliminary studies indicate that there is a positive role of both CB1 and CB2 receptors. It is highly probable that the production and metabolism of endogenous cannabinoids and its associated signaling become impaired during the disease. But the receptors’ level remain almost the same. So, particularly CB1 becomes the major focus and the target for this disease. For a limited time, positive results regarding the behavior have been noticed by administering Δ9 – THC or any of its analogs. The activation of CB1 and CB2 offers neuroprotection against Amyloid-β toxicity which is previously observed in several neurodegenerative diseases. The receptor activation reduces dementia simultaneously enhances the cognitive repair due to anti-inflammatory actions of cannabinoids. Additionally, cannabidiol / CBD prevents phosphorylation of Tau protein which is also another indication of neuroprotection.
Effect on Huntington’s disease (HD): It is also called Huntington’s chorea. It is an inherited neurological disorder created due to the autosomal dominant mutation in either of the parents which causes death of brain cells. HD creates lack of coordination, unsteady or jerky body movement, lowering the motor performances and subsequent production of dementia. Improper utilization of endocannabinoids is noticed according to the animal models. The expression of CB1 receptor mRNA decreases ~ 27% inside striatum that leads to the loss of motor performances and simultaneously enhances the neuronal aggregation. Identical phenomena are also noticed within the humans suffering from HD. The activation of CB1 receptor by Δ9 – THC plus CBD / Sativex (Novartis) enable to reduce the progression of disease. Other selective CB1 agonists are also noticed to be effective for neuroprotection. According to the animal and cellular model, activation of Gαi/o mediated pathways limiting the release of glutamate from cortical neurons could be a part of the reasons. Additionally, CB1 activation also enhances the expression of BDNF which also provides neural protection. Thus, selective CB1 agonists can be used in the treatment of HD.
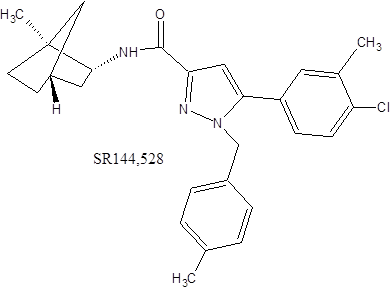
Immune modulation and effect on tumor suppression: Most of the cannabinoids, Δ9 – THC, CBD, cannabinol including the endogenous products eg, anandamide, 2- Arachidonyl glycerol and Arachidonyl ethanol amine and synthetic agonists are seen to impose strong immunomodulatory effects. Those induce apoptosis in human lymphocytes / PBMC preventing cellular proliferation by acting as immunosuppressive agents by lowering Bcl-2 leading to the reduction of IL-1. The anti-tumor effect is linked to its induction of apoptosis. Animal experiments showed that intra-tumor injection of Δ9 – THC, WIN55, 212-2 and others showed significant recession of gliomas. In cultured C6 gliomas, cannabinoids can induce apoptosis via the CB2 receptors. Similar effect is observed using specific CB2 agonist, JWH-133, which is inhibited by the selective antagonist SR144528 (Sanofi). Both endo-cannabinoids and cannabinoids either synthetic or plant derived can inhibit human breast cancer cells. It works via CB1 receptor while downregulating large form of Prolactin receptor. Cannabinoids are involved in suppressing the tumor growth in multiple ways eg, inducing accumulation of lipid droplet within the cells or by suppressing the angiogenesis. Besides those a large number of human cancer cell lines undergo apoptosis by the action various cannabinoid agonists. Therefore agonist action targeting the receptors using various cannabinoids could be the potential strategy to control numerous proliferating tumors.
Remarks: Cannabis is in use for more than millennia whether for recreational, religious or medicinal reason is not exactly known. In India, religious label is associated with the marijuana use for Hindu religion which is presumably due to the psychoactive effect. For the sake of transitory hallucinogenic effect, the herb has been abused as a trip to pleasure. Medical studies have proven that cannabis imposes psychosis, creates accidents, unwanted sexual encounters and aggressive behavior. The chronic use often induces attention deficit and hyperactivity disorder (ADHD), disorderly conduct and learning disorders. Despite the immense adversarial effects, medicinal values of cannabis are enormous. The plant is a large source of chemical compounds that offer multitudes of beneficial health effects acting as analgesic, neuroprotective, anti-inflammatory, anticonvulsant, appetite stimulator, anti-emetic also protecting from other diseases. The discovery of endo-cannabinoids facilitates the cannabis research further along with identification of its receptors (CB1 and CB2) expressing in neuronal and non-neuronal tissues. Following that course, a myriad of drugs has been synthesized particularly for those suffering from the neuronal disorders.
